Thermal burn - symptoms and treatment
Medical care for burn injuries is currently subject to the order of the Ministry of Health of 1991 No. 54 “On measures for the further development and improvement of medical care for burn victims.”
First aid for thermal burns
For patients with burns, first aid should be provided immediately at the scene of the accident.
- First you need to stop the action of the thermal agent:
- extinguish the flame on clothing;
- remove the victim from the high temperature area;
- remove smoldering clothing or clothing soaked in hot liquid if it is not soldered to the wound surface. If the tissue is stuck, you need to carefully trim it around the wound.
- In the first 10-15 minutes from the moment of injury, you need to cool the burned surface: for 1st and 2nd degree burns - with cold running water for 10-15 minutes; for a 3rd degree burn, apply a cold, damp, sterile bandage or clean cloth. This will significantly reduce the effect of the thermal agent and stop it from spreading deeper into the tissue. This procedure also reduces swelling and pain. All these points have a beneficial effect on further wound healing.
- Before emergency medical services arrive or before you consult a doctor yourself, it is recommended to perform a dressing using sterile gauze pads or clean sheets.
What not to do for burns
In case of burns, you should not:
- Carry out any manipulations on the wounds.
- Prick or try to remove blisters.
- Use ice to cool the burn area, as it can lead to additional injury - frostbite.
- Separate stuck objects.
- Tearing off the stuck tissue will further injure the victim and cause additional pain.
, it is not recommended to use various powders, ointments and sprays as first aid for burns They can make it much more difficult to determine the depth of the lesion and clean the wound.
Treatment of burns with folk remedies
It is not recommended to use traditional medicine methods such as toothpaste, sunflower oil, diluted boric acid, urine, etc.
It is important to remember that only specialist doctors (surgeons, combustiologists, traumatologists) can provide qualified medical care. Self-diagnosis and self-medication can be dangerous to health [5][9].
When to call an ambulance for a burn
An ambulance should be called in the following cases:
- with deep burns or if their size is larger than the victim’s palm;
- the skin in the burn area is charred or whitened;
- blisters appeared;
- there are other injuries;
- the patient is in a state of shock - trembling, sweating profusely, his skin becomes sticky, breathing quickens, weakness or dizziness appears;
- the victim is pregnant;
- patient under 5 or over 60 years of age;
- the person is known to have heart disease, lung disease, liver disease or diabetes, or has a weakened immune system, for example due to HIV, AIDS or chemotherapy for cancer;
- the victim inhaled smoke, which causes a cough, sore throat, difficulty breathing, and noticeable burns on the face [19].
Outpatient burn treatment
The frequency of visiting the doctor depends on the severity of the burn. In mild cases, the first visit is scheduled a day after the injury, then you need to visit the doctor about once a week. At the appointment, the doctor treats the wound, assesses the depth of the burn and the need for skin grafting.
If an infection is associated with the burn, then you need to visit a doctor as soon as possible. When a wound becomes infected, adjacent areas of the skin turn red, pus is released intensely, and black or red spots appear in the burn area.
During outpatient treatment, it is important to keep the burn surface clean. The doctor may prescribe ointments that are applied to the wound and then covered with a dry gauze bandage. The dressing should be changed daily. Biosynthetic dressings do not need to be changed if there is no suppuration [20].
Treatment of burns in hospital
Treatment for burn injuries is consistently one of the most expensive. Treatment methods for patients with thermal injuries are now fundamentally different from those generally accepted 10-15 years ago. Modern algorithms for the treatment of burn wounds have been developed largely due to advances in the study of burn disease. The results of treatment of patients with burns have improved significantly due to the development and implementation of active surgical tactics in clinical practice. The basis is early necrectomy followed by skin grafting in order to quickly restore the integrity of the entire skin.
The essence of necrectomy is the excision of non-viable tissue using a scalpel and/or special equipment (hydrosurgical scalpel, dermatome). This is necessary to prepare the wound for closing the defect. If the wound area is small, it is possible to perform autodermoplasty (skin grafting) with local tissue. If the affected area is large, autodermoplasty is performed with a free skin flap, i.e. using one’s own areas of unaffected skin. The skin graft is harvested under general anesthesia using a special instrument - a dermatome. The thickness of the flap is usually 0.3-0.4 mm. Then it is placed on the wound surface, fixing the edges with sutures or metal staples [5].
Innovative methods for diagnosing and treating children with burn injuries include determining the depth of the burn, active debridement (surgical treatment of wounds), and treatment of wounds with negative pressure. The modern approach to the treatment of burn wounds is carried out through the earliest possible preparation for autodermotransplantation [16].
The most effective from a modern point of view is cleansing the wound surface from necrotic masses using hydrosurgical systems . Their main principle is the ability to carry out operations without tools, using a special solution that moves at great speed. The jet in pulsation mode provides cleaning and treatment of wounds, and also makes it possible to excise tissue. The system removes tissue fragments formed during wound cleaning [11]. The hydrosurgical system allows surgeons to set the desired mode and treat even complex wounds as efficiently as possible, with the formation of the desired edge configurations.
Currently, the use of a negative pressure apparatus . The essence of this method is to create a controlled local subatmospheric pressure, i.e., a vacuum, directly in the wound. A constant or variable level of negative pressure is created using a special dressing that isolates the wound surface from the external environment [4]. Vacuum therapy has already received comprehensive scientific substantiation and recognition among specialists in the field of treatment of wounds of various etiologies.
When treating children with burn injury, it is important to pay attention not only to the wound surface itself, but also to the psychological state of the child himself and the relatives caring for him (most often the mother). The mother’s task at the stages of treatment and rehabilitation is to help minimize physical and psychological disorders in the child.
Treatment of deep and/or extensive burns requires long-term hospitalization (about 2-3 months or more). Then comes the rehabilitation period, which can last for years. Typically, recovery, like treatment, includes financial costs [1][6][7]. All this negatively affects the psychological state of the mother.
The longer the victim’s mother experiences physical and mental exhaustion, the worse the prognosis for the child’s long-term adaptation [3][10]. In order to reduce chronic stress and develop adaptive abilities in mothers, individual or group psychotherapy is recommended [8]. Family therapy should be included in the rehabilitation treatment of burned children [2][10].
Burns in children
Burns in children are a type of injury that occurs when tissue is damaged by physical and chemical factors (thermal energy, electricity, ionizing radiation, chemicals, etc.). The clinical picture of burns in children depends on the factor involved, the location, depth, and extent of tissue damage and includes local (pain, hyperemia, swelling, blistering) and general manifestations (shock). The main tasks of diagnosing burns in children are to determine the nature of the burn injury, the depth and area of damage, for which infrared thermography and measuring techniques are used. Treatment of burns in children requires anti-shock therapy, cleaning the burn surface, and applying bandages. Symptoms of thermal burns in children
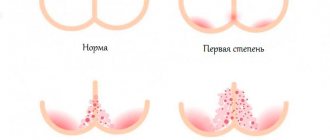
Depending on the depth of tissue damage, thermal burns in children can be of four degrees.
A first degree burn (epidermal burn) is characterized by superficial damage to the skin due to short-term or low-intensity exposure. Children experience local pain, hyperemia, swelling and a burning sensation. At the site of the burn, slight peeling of the epidermis may be observed; superficial burns in children heal in 3-5 days on their own without leaving a trace or with the formation of slight pigmentation.
A second degree burn (superficial dermal burn) occurs with complete necrosis of the epidermis, under which clear liquid accumulates, forming blisters. Swelling, pain and redness of the skin are more pronounced. After 2-3 days, the contents of the bubbles become thick and jelly-like. Healing and restoration of the skin lasts about 2 weeks. With second degree burns in children, the risk of infection of the burn wound increases.
A III degree burn (deep dermal burn) can be of two types: IIIa degree - with preservation of the basal layer of the skin and IIIb degree - with necrosis of the entire thickness of the skin and partially the subcutaneous layer. Third degree burns in children occur with the formation of dry or wet necrosis. Dry necrosis is a dense scab of brown or black color, insensitive to touch. Wet necrosis has the appearance of a yellowish-gray scab with a sharp swelling of the tissue in the burn area. After 7-14 days, the scab begins to be rejected, and the complete healing process is delayed for 1-2 months. Epithelization of the skin occurs due to the preserved germ layer. IIIb degree burns in children heal with the formation of rough, inelastic scars.
A IV degree burn (subfascial burn) is characterized by damage and exposure of tissues lying deeper than the aponeurosis (muscles, tendons, blood vessels, nerves, bones and cartilage). Visually, with fourth degree burns, a dark brown or black scab is visible, through the cracks of which the affected deep tissues are visible. With such lesions, the burn process in children (wound cleansing, formation of granulations) proceeds slowly, local, primarily purulent, complications often develop - abscesses, phlegmon, arthritis. IV degree burns are accompanied by a rapid increase in secondary changes in tissues, progressive thrombosis, damage to internal organs and can result in the death of the child.
Burns of I, II and IIIa degrees in children are regarded as superficial, burns of IIIb and IV degrees - as deep. In pediatrics, as a rule, there is a combination of burns of various degrees.
Treatment of burns in children
To treat burn shock in children, various types of anesthesia are used (omnopon, pipolfen; chloral hydrate, nitrous oxide, etc.) with simultaneous restoration of the volume and composition of circulating blood. In severe cases, it is recommended to use a lytic mixture consisting of largactil, phenergan and dolantin. The child should be kept warm. Most pediatric surgeons insist on limiting parenteral fluids. During the first day of the disease, blood or its substitutes are administered at the rate of 1.5 ml per 1 kg of the patient’s weight and 1% of the burnt surface and 1 ml of physiological sodium chloride solution per 1 kg of weight and 1% of the burn surface. If there is no vomiting, drink plenty of fluids.
First aid for burns in children involves stopping the action of the thermal agent, freeing the affected area of skin from clothing and cooling it (by washing with water, an ice pack). To prevent shock at the prehospital stage, the child can be given analgesics.
In a medical institution, the child undergoes primary toileting of the affected area under general anesthesia. Foreign objects are removed from the wound by treating the edges of the wound with an antiseptic. If the skin is preserved, it is placed on the affected surface to reduce pain and speed up wound healing. The surface of the wound is lubricated with sterile petroleum jelly. Further treatment tactics are possible in two ways: open and closed treatment. Open treatment is preferable in older children. This method is less painful, but it is necessary to create certain conditions in the observation room and strict asepsis to prevent infection from entering the wound.
With the closed method of treatment, a sterile bandage is applied to the wound, which is changed as necessary depending on the depth and area of the lesion. When changing the dressing, clean the wound and lubricate the surface of the affected area with antiseptic and healing ointments.
For deep burns, surgical treatment is indicated to restore the integrity of the skin, as this is the key to recovery.
The dead tissue is excised and the defect is closed with a skin flap. Surgical treatment is carried out in stages, sometimes requiring up to 10 surgical interventions. ov in children is determined by a surgeon-combustiologist or a pediatric traumatologist.