Anatomy of permanent teeth
Each molar consists of certain parts:
- crown. This is the part of the tooth that protrudes from the top;
- the root, it goes deep into the alveoli. At the same time, it is attached thanks to special connective tissue bundles. There can be different numbers of roots (1-5 pieces). This moment affects the number of nerves and channels;
- neck. This part is located between the root and the crown.
Tooth tissues are distinguished by their heterogeneity. The enamel is on top and is known for its durability. Once the tooth has erupted, it is covered with a transparent thin layer. This is the cuticle, which eventually changes to the pellicle. The latter is a film that is created from what saliva produces.
Beneath the enamel is dentin, the tissue of the tooth. Dentin is similar to bone when you study how it is built. However, it is more durable because there is a high level of mineralization. In the area where the root is located, the dental tissue is covered with cement. The latter is rich in mineral compounds and is also associated with periodontium. Collagen fibers are used for this.
As for the part of the tooth that is inside, this is the crown and root canal. They are filled with pulp. This is loose connective tissue; it contains nerve endings and blood vessels.
Differences between baby teeth and permanent teeth
Permanent and temporary teeth are built in the same way, but still have certain differences between themselves:
- The enamel on baby teeth is whiter. And the enamel on permanent teeth has a yellowish tint;
- the best indicators of density and mineralization are noted behind the molars;
- the pulp of a baby tooth is large in size, and the dense tissues and their walls are thinner;
- permanent teeth are larger in size, here the length is greater than the width;
- The root of baby teeth is short and thin compared to permanent teeth. When the root of temporary teeth is formed, they expand in width. Therefore, the permanent bud has free space to grow.
Causes of delayed eruption of permanent teeth –
If for baby teeth delayed eruption is considered to be a delay of only 2-3 months, then for permanent teeth this figure is already 2-4 years. Among the main reasons for the delay in the eruption of permanent teeth, it is particularly worth highlighting the preceding inflammatory processes in the area of the roots of primary teeth, as well as the early removal of primary molars.
1) Violation of local conditions for teething:
- underdevelopment of the upper and lower jaws,
- lack of space in the dentition,
- premature removal of primary molars,
- incorrect position of the tooth germ,
- tooth germ injury,
- inflammation in the bone tissue of the jaws, for example, with purulent periodontitis of baby teeth.
2) Common causes of delayed eruption of permanent teeth:
- rickets or congenital syphilis,
- exudative diathesis,
- various chronic intoxications,
- metabolic disorders,
- disturbances of reflex-trophic processes,
- hormonal imbalances (for example, hypothyroidism, hypofunction of the thymus or adrenal glands).
Which permanent teeth are more likely to experience delayed eruption?
- one of the canines of the upper jaw (MF) – occurs in 43.64% of children,
- two HF fangs at once – in 25.65%,
- second premolar of the mandible (MF) – in 12.84%,
- two HF canines and LF second premolars at once – in 10.34%,
- both second premolars LF – in 5.11%,
- both lateral incisors HF – in 2.61%.
Where do teeth come from?
Teeth begin to form and develop when the fetus is still inside the womb (at about 6 weeks). They have their source - the epithelial dental plate. Already by 14 weeks, active formation of dental tissues, which are hard, occurs. Initially, this occurs in the area where the crown will be, and later at the root.
Molars, namely their first rudiments, appear by the 5th month of the embryo. They are located higher than the child’s baby teeth or lower. By the time the child is born, the rudiments are already practically formed in the tissues of the jaw.
Teeth that belong to an additional group (have no predecessors) are formed later. This occurs after about 1 year of life. Why? Because the baby's jaw is still very small and there is not enough space for them.
Symptoms of teething in children
Signs of teething in infants can be observed already 3-5 days before teething. Symptoms continue until the crowns of the teeth appear through the mucous membrane of the gums. The main symptoms of teething in infants are:
- redness and swelling of the gums at the site of eruption,
- irritability,
- bad dream,
- poor appetite, refusal to eat,
- the child tries to bite whatever he can, trying to relieve the itching in the gums,
- increased salivation and drooling,
- rash and irritation in the mouth and chin area, as well as on the chest
(occur due to drooling from the mouth).
→ Homeopathic remedies for teething
→ Pain-relieving gels for topical use
Additional signs of teething in children:
- How long does the temperature last during teething in children?
In most children, teething does not lead to an increase in temperature. High temperature is usually a consequence of some concomitant inflammatory process unrelated to teething. For example, it may increase against the background of ARVI, or against the background of herpetic stomatitis of the oral cavity (the latter is characterized by the symptoms described below).It is worth carefully examining the mucous membrane of the child’s oral cavity for the presence of - 1) small blisters filled with clear or cloudy liquid, 2) small erosions surrounded by inflamed bright red mucous membrane, 3) bright red inflamed gums. In a 1-year-old child, antibodies to the herpes virus received from the mother during pregnancy gradually disappear, and trauma to the mucous membrane from teething is a trigger for the development of viral stomatitis.
- Hematomas on the mucous membrane of the gums (Fig. 8) -
in some children, 2-3 weeks before teething, a lump filled with clear or bluish liquid may appear on the gum. This does not indicate inflammation or any pathology, and usually does not require intervention (only if this formation has reached too large a size, a small incision is made to release the bloody fluid).
- Coughing and vomiting during teething –
increased salivation is observed during teething, and if the child has swallowed saliva, then such symptoms may be present. If vomiting occurs against the background of a high temperature or abnormal stool (diarrhea), then teething has nothing to do with it. In this case, you should immediately suspect rotavirus and urgently call a pediatrician home.
Important: we repeat once again that high fever, vomiting and diarrhea cannot in any way be associated with teething. Their causes are intoxication of the body against the background of a concomitant infectious process (influenza, ARVI), rotavirus infection. In these cases, you should definitely call a pediatrician.
If you find herpetic rashes (vesicles, erosions) on the mucous membrane of the child’s mouth, or all the gums are bright red, then this is typical for herpetic gingivostomatitis. In this case, it is better to call a pediatric dentist from a pediatric dental clinic at your place of residence, because Pediatricians in most cases do not know that there are several forms of stomatitis, each of which is treated differently.
What does a dental formula look like?
To make it more convenient to describe teeth and their number, special formulas are usually used. Each tooth has its own number, which is used to decipher its location.
When describing a milk bite, Roman numerals are used:
- incisors – I, II;
- canine – III;
- molars – IV, V.
If we talk about the formula for adult teeth, here the teeth are counted starting from the center:
- incisors – 1.2;
- fang – 3;
- molars (small) – 4.5;
- molars (large) – 6,7,8.
8 is a wisdom tooth; not every person has it.
Teething order
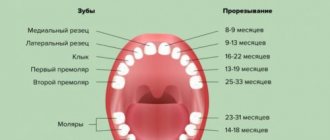
Typically, all children start teething at about the same time. Teeth emerge from the molar set at the age of 5, and it is the molars (large ones) that emerge. Then the diagram is as follows:
- Initially, the incisors on the lower jaw change, which are located in the center;
- then the central incisors appear on the upper jaw and the incisors on the sides on the lower jaw;
- at about 8-9 years old, the incisors on the top and sides change;
- up to 12 years of age, molars (small) grow;
- at the age of 13, the fangs change;
- after the child turns 14 years old, the second molars (large ones) come in. They were not included in the milk kit;
- and after another 1 year the third molars (large) appear. This is a wisdom tooth. But he may not appear at all.
Diagram of teething of primary occlusion
A newborn child has 20 primary tooth buds inside the upper and lower jaws (10 follicles for each jaw). The timing of teething in children, according to different authors, can vary greatly, and in diagram No. 1 below you can see generally accepted figures from the “National Guide to Pediatric Dentistry”. In this diagram you can see the timing of the eruption of baby teeth in completely healthy children who do not have any pathology.
Scheme of teething in children without pathology (scheme No. 1) –
According to statistics, the normal schedule for teething in children is observed only in 42% of cases. A delay in the timing of eruption is observed in approximately 48% of children, which is associated with illnesses suffered - both by the mother during pregnancy and by the newborn child (you can read about the main reasons for the delay in eruption below). Approximately 10% of all children experience early eruption of primary teeth, and in a small percentage of cases this can occur even during fetal development.
What may cause delayed teething?
Many factors can influence the delay in the eruption of primary teeth. For example, in premature children with general somatic pathology, the eruption of the first teeth in 61% of cases occurs only at the age of 8 months and older. Moreover, if a premature baby has suffered an intracranial birth injury or a severe infectious-inflammatory disease, then eruption may begin even later - at 11-12 months and older.
The timing of the onset of teething also depends on the duration of natural feeding. In bottle-fed children, in 60% of cases, the first temporary teeth erupt only at 8 months or later. In mixed-fed children, delayed eruption was observed in only 30% of cases. A lot depends on the state of health of the mother during pregnancy, as well as on the course of pregnancy. For example, when examining children under 3 years of age whose mothers suffered severe toxicosis, it was found that the start of the eruption of primary teeth in them shifted to 8-10 months.
It is also worth noting that delayed eruption in a small percentage of cases can occur even in completely healthy children, which is associated with a genetic factor (for example, when late eruption was observed in one of the child’s parents). The “National Guide to Pediatric Dentistry” published a table that clearly shows what the delay in eruption may be if a child has various diseases.
Table No. 1 - timing of the onset of eruption in the presence of pathology
List of reasons for delayed eruption of baby teeth:
1) The first group of reasons includes diseases of a woman during pregnancy, as well as features of the course of pregnancy. Moreover, it is worth noting that all these reasons have only a moderate effect (unlike diseases in the 1st year of a child’s life). These reasons include:
- toxicosis of the 2nd half of pregnancy,
- kidney disease,
- previous pneumonia or acute respiratory infection with high fever,
- herpes infection, rubella, toxoplasmosis,
- constant chronic or short-term severe stress.
2) The greatest influence on the delay in the eruption of baby teeth is caused by diseases suffered during the 1st year of the child’s life:
- neonatal sepsis,
- pneumonia, frequent acute respiratory infections,
- atopic dermatitis, rickets,
- general somatic pathology,
- convulsive states,
- intestinal toxicosis,
- prematurity and postmaturity,
- hypothyroidism (lack of iodine intake),
- poor unbalanced diet,
- for epilepsy.
Causes of early teething: studies have found that early teething is most often characteristic of children born with a large body weight. Moreover, there is a clear correlation - the greater the child’s body weight, the earlier the eruption of temporary teeth begins. Also, premature eruption is observed with adrenal tumors accompanied by hyperfunction (24stoma.ru).
Violation of the sequence of teething in children -
Physiological teething is characterized not only by timing, but also by such characteristics as pairing and sequence. Those. all teeth should erupt in pairs, for example, first 2 central incisors of the lower jaw erupt at once, then 2 central incisors of the upper jaw, etc. See diagram No. 1 above for the timing and sequence of baby teeth eruption. In healthy children, there are usually no violations of pairing and sequence during teething.
But in children who have suffered from rickets, sequence violations occur in approximately 52% of all cases, pairing disorders occur in approximately 35% of cases. In children with rickets, the eruption of primary teeth very often begins with the central and lateral incisors of the upper jaw, and when the crowns of the teeth erupt approximately halfway, the eruption process may stop for many months. The latter is associated with a violation of the formation of the roots of milk teeth, because when milk teeth just begin to erupt, their roots are still only 25-50% formed.
How to determine that a child will soon have molars?
There are certain signs that indicate that permanent teeth will soon begin to erupt:
- The spaces between the teeth increase. The jaw grows and the free space increases;
- baby teeth become loose as the root gradually dissolves. It cannot be firmly fixed in the jaw tissues;
- in case of loss of a temporary tooth. This confirms that the molar will soon come out as it has pushed out the previous one;
- The gums are slightly swollen and red.
When permanent teeth erupt, the child’s general well-being usually remains the same, the temperature does not rise, and there is no pain.
Possible problems
Permanent teeth have just appeared, but this does not mean that there will not immediately be any problems associated with them. Parents should be aware of possible dental problems:
- lack of molars;
- pain in the molar area;
- crooked position of molars;
- molars fall out;
- injuries.
For any of these problems, it is important to contact a specialist in time to receive qualified help.
If your child has a fever
A temperature of 37 degrees is considered normal; up to 37.5 this will also not be considered a special or complicated situation. Children usually feel fine with such a slight increase in temperature. Naturally, there is no point in giving an antipyretic in this case.
If the temperature rises above 38 degrees, it is worth saying that inflammation or infection has joined the teething process. This situation requires seeing a doctor (he needs to be called to your home), and only his recommendations will be your tactics in future behavior.
During this period, children experience pain, malaise, and weakness that were not typical before, so their behavior changes, sleep disturbances and refusal to eat are noted, which only aggravates the temperature reaction. First of all, the child needs rest, calm and healthy sleep, because temperature, on the one hand, is a protective reaction, and on the other, a debilitating process, which, if unfavorable, can cause overstrain of all organs and systems with the development of pathological reactions: weakness, drowsiness, tachycardia and even febrile seizures.
And remember that the antipyretic should be strictly for children, ideally recommended by a doctor. These are usually paracetamol-based drugs. If they do not help, you can give the child Ibuprofen (but it is prescribed to children from one year old).
But under no circumstances should children be given medications of the aspirin and analgin group. These are toxic drugs that cause side effects.
An excellent tactic for high temperatures would be to humidify the air in the room, regularly ventilate (while the child is in another room), drink plenty of fluids and eat as desired. The child should drink a lot of warm drinks and eat only when he wants to. Avoid dry air, wrapping yourself up in three pajamas and two blankets. If a child wants to play at a high temperature, there is no need to force him to go to bed.
It is important to understand that if the temperature is elevated for more than three days, it is unlikely that the problem is teething. And when it still doesn’t go astray, urgently call a doctor and look for the real reason for this reaction of the body.
Teething is not a very long period. By the age of three, it is definitely completed, and then you will already wait for the loss of milk teeth and the growth of permanent ones. As a rule, the child tolerates these processes normally. To make sure everything is in order, visit your pediatric dentist every six months. You can take care of baby teeth from the moment they appear. Teach your child to brush his teeth twice a day, monitor the quality of brushing.