Parents usually closely monitor all changes in the condition of their newborn baby. This allows you to find out about the onset of the disease in time and prevent the development of complications. The baby can only communicate with his parents by shouting: his crying is a signal of a problem. Perhaps the child is hungry, he lacks communication, the diapers urgently need to be changed, the baby has a tummy ache or something else. If a baby has a hoarse voice, you should know what causes this symptom. Why does a baby’s crying suddenly change in timbre, how dangerous is it and what should parents do? You will find detailed answers to these questions in this article!
Why is my voice hoarse?
A hoarse voice in a baby can occur for the following reasons:
- The baby cries too long and often. If the ligaments are strained for a long time, the vessels supplying blood to the oropharynx can be damaged. As a result, swelling occurs, which makes the voice hoarse;
- a hoarse voice in a baby may occur due to the presence of any neoplasms in the pharynx, for example, papillomas;
- inflammatory diseases of the larynx. Parents may notice that the baby is hoarse if the child has contracted a bacterial or viral infection. At the same time, symptoms such as fever, cough, decreased appetite, anxiety and moodiness, and bowel dysfunction may be observed;
- injuries to the neck and throat area. In this case, a hoarse voice may be accompanied by a change in the position of the child’s head, bruises on the front or side of the neck.
Frequent and prolonged crying is one of the reasons for a child’s hoarse voice
Reasons why the voice disappears
The voice may not completely disappear (this is called dysphonia); more often we are faced with hoarseness or hoarseness. Complete aphonia with the ability to speak in a whisper is observed relatively rarely. Causes of this symptom:
- infection - most often voice changes occur with tonsillitis, pharyngitis, laryngitis;
- anomaly of the development of the larynx - in this case, dysphonia is detected during the neonatal period;
- allergies - swelling of the larynx and vocal cords;
- benign and malignant tumors of the larynx;
- myasthenia gravis;
- hormonal diseases;
- injuries (a long scream is also an injury);
- damage to the cranial nerves or their centers, etc.
In all these cases, the voice may become nasal, hoarse, quiet, hoarse, or completely disappear.
Situations requiring emergency assistance
Hoarseness in a small child, especially an infant, may be a signal that it is necessary to urgently seek medical help. Parents should immediately take control of the situation in the following cases:
- Hoarseness in an infant is caused by the penetration of a foreign body into the respiratory tract. For example, a baby may choke while eating, inhale a small part of a toy, etc. In this case, there is a serious danger to the baby’s life: an infant quickly develops hypoxia, which is manifested by blue skin, severe coughing or pallor. If parents suspect that the child is choking, they should immediately examine the throat for the presence of a foreign body and try to remove it;
- laryngeal stenosis. This condition is observed if a child quickly develops an allergic reaction such as Quincke's edema, or, as it is also called, angioedema. At the same time, parents may note that the child not only has lost his voice, but also swelling of the face, neck and limbs is rapidly increasing. Quincke's edema is a serious condition that can lead to suffocation and death, so it cannot be treated at home. Angioedema in an infant should be treated in a hospital setting;
- false or true croup. With these diseases, the larynx becomes inflamed and narrows, resulting in significant difficulty in breathing. If treatment is not started promptly, the child may suffocate. Most often, croup occurs in children aged three months to two years. Symptoms such as hoarseness, difficulty breathing, blue discoloration of the nasolabial triangle and the upper phalanges of the fingers indicate croup. In severe cases, the child may lose consciousness due to lack of oxygen. Naturally, treatment for croup must begin as early as possible and only a doctor can prescribe a suitable treatment regimen.
Hoarseness in Children
Voice is a unique tool for interpersonal communication. Voice quality is of utmost importance due to the complexities associated with social development and social adaptation. At the same time, voice disorders among school-age children range, according to various sources, from 6 to 23% and are increasing every year. Since communication skills play an important role today, the function of phonation in a child is becoming an increasingly important issue. Voice disorders can mainly be divided into qualitative disorders (dysphonia), resonance pathology (hypernasality, hyponasality), timbre and loudness disorders.
The structure of a child’s larynx has some peculiarities. The high position of the larynx allows the baby to breathe and swallow at the same time. However, the relatively flat base of the skull and the high localization of the larynx (in a newborn - at the level of 3-4 cervical vertebrae, dropping to the level of 6-7 cervical vertebrae by the age of 15) cause a certain “inadequacy” of phonation space in children. The child's pharynx has a conical shape, becoming cylindrical in adults, which causes a decrease in the formant frequency of the voice. The length of the vocal folds in a newborn is usually from 6 to 8 mm and increases by adolescence to 12-17 mm in girls and 17-23 in boys; at the same time, the most rapid growth of the structures of the larynx is observed in the puberty period, especially in boys, which leads to the formation of a lower voice in them (the frequency of a cry in a newborn is 400-600 Hz, halving by the age of 8-10 years and to 50 Hz in boys adolescence).
Diagnosis of voice disorders requires a multidisciplinary approach; in this case, the main role is played by the otorhinolaryngologist and speech therapist; in some cases, additional consultation with a pediatrician, neurologist, gastroenterologist, allergist, pulmonologist, medical geneticist, endocrinologist and other specialists may be required. It is necessary to find out not only the age at which voice disorders first appeared and their possible causes, but also a history of head and neck injuries, and especially intubation, the presence of bronchial asthma, gastroesophageal reflux, neurological disorders, etc.
Endoscopic examination plays a leading role in the diagnosis of voice disorders. Indirect (mirror) laryngoscopy, stroboscopy and examination of the upper respiratory tract using rigid endoscopes, widely used in adults and adolescents, are practically impossible to use in newborns and young children. In this regard, the most effective method of visualizing the larynx in childhood is fiber endoscopy, during which it is possible to assess the condition of the nasal cavity, nasopharynx, laryngopharynx and all structures of the larynx. It should be taken into account that the child is not capable of prolonged phonation, which greatly complicates the stroboscopic examination of him. Microlaryngoscopy under anesthesia may be required in the following cases:
- to examine the larynx if fibrolaryngoscopy is difficult or impossible;
- in children with increased emotional excitability or mental retardation;
- for a detailed examination of the larynx if there is a suspicion of a congenital or acquired anomaly of the structure of the larynx;
- if it is necessary to carry out diagnostic and therapeutic manipulations in the larynx.
Changes in crying in newborns are characteristic of many pathological conditions, both congenital (cry the cat syndrome, Down syndrome, Williams syndrome, Simpson-Golabi-Bemel syndrome, Jadosson-Lewandowski syndrome, Pfeiffer syndrome, etc.) and acquired origin (encephalitis, meningitis, hyperbilirubinemia, various pathological conditions of the central nervous system). In particular, hoarse crying is usually caused by inflammatory diseases of the airways or damage at the level of the vocal folds. A high-pitched cry is characteristic of infants with central nervous system damage. A weak voice is found in children with muscular dystrophy.
The most common anomaly of the larynx, laryngomalacia, does not in itself cause a change in voice, but may be accompanied by other developmental anomalies and gastroesophageal reflux (see below), leading to hoarseness.
Congenital vocal fold paralysis is clinically manifested by dysphonia and stridor. In most cases, the paralysis is unilateral; the left vocal fold is most often affected. Unilateral paralysis usually does not require surgical intervention and, compared to congenital bilateral paralysis, recovers spontaneously more often. The need for tracheotomy usually arises in cases of bilateral vocal fold paralysis, and it is advisable to postpone reconstructive operations until the child reaches 5-6 years of age, since the lost function is often restored. With bilateral vocal fold paralysis in an infant, a thorough diagnosis of possible diseases of the central nervous system, including tumors, is necessary.
Congenital synechiae of the larynx (anterior commissural membranes) are a fairly rare pathology. In the vast majority of patients, the first symptom of a developmental anomaly is a change in voice: “cock crow” or hoarseness. Considering the high frequency of detection of syndromic pathology and multiple malformations in children with congenital laryngeal synechia, such patients require a comprehensive examination. Small membranes (narrowing the lumen by 1/3 or less) do not require surgical intervention; in this case, only phonopedic treatment is indicated upon reaching 6-7 years of age. Larger synechiae cause, along with dysphonia, the phenomenon of respiratory stenosis, requiring urgent surgical treatment, including tracheotomy.
Among diseases of the endocrine system that lead to dysphonia, hypothyroidism, hypoglycemia and hypertestosteronemia are more often found.
The etiology of acquired dysphonia is infectious, traumatic, neoplastic, psychogenic, and endocrine in origin. Along with acute laryngitis of an infectious nature, the most common are vocal fold nodules (“singing nodules”), cysts, and polyps. In recent years, it has been discovered that gastroesophageal reflux is also important in the development of dysphonia.
Gastroesophageal reflux can cause dysphonia in children due to direct irritation of the larynx (reflux laryngitis). Although the association of vocal fold nodules with gastroesophageal reflux has not been proven, chronic inflammation of the vocal folds caused by reflux can lead to the formation of nodules. The diagnosis of gastroesophageal reflux can be made based on the results of fluoroscopy of the esophagus with contrast or 24-hour pH monitoring. Contrast fluoroscopy of the esophagus is not informative enough due to the short duration of the study. The “gold standard” for diagnosing gastroesophageal reflux is 24-hour pH testing of the esophagus, which allows one to determine the duration and frequency of reflux episodes. Indirect signs of extraesophageal reflux can be an increase in the lingual tonsil, swelling and hyperemia of the mucous membrane of the arytenoid cartilages, posterior parts of the vocal folds, subglottic part of the larynx, trachea and even tracheal bifurcation, detected by direct microlaryngoscopy and tracheobronchoscopy.
Viral laryngitis is the most common cause of acute hoarseness in children. Another acute viral disease, clinically manifested by hoarseness and stenosis of the respiratory tract (up to asphyxia), is epiglottitis, the etiological factor of which in most cases is the Haemophilus influenzae virus, type B.
Vocal cord nodules are one of the most common causes of dysphonia in children. Children with “singing” nodules are characterized by such behavioral reactions as loudness, increased excitability, aggressiveness, emotional lability; in this regard, children with such pathology first of all need correction of their behavioral reactions. In addition, such patients are indicated for more “aggressive” treatment of possible concomitant pathology of the central nervous system compared to other children. In most cases, vocal fold nodules in children self-destruct during puberty. Treatment tactics for children with nodules depend on the severity of dysphonia, and it is necessary to take into account the possible negative psychological aspects of surgical treatment. Generally, surgical removal of nodules is indicated for children who need immediate improvement in their voice or for large nodules; in all other cases, it is advisable to use voice therapy, phonopedic treatment, resorting to surgical intervention only if phonopedic classes are ineffective in older children against the background of complete neurological and psychological correction.
Based on the vast majority of observations, the isolated use of phonopedic therapy in children with polyps or cysts of the vocal folds has been found to be ineffective. In children with such pathology, it is advisable at the first stage of treatment to surgically eliminate the formation followed by phonopedic treatment.
Acquired paralysis in children is usually caused by injury to the recurrent nerve during operations on the mediastinal and thoracic organs. With unilateral paralysis, as a rule, there is hoarseness without pronounced respiratory stenosis; with bilateral dysphonia is less pronounced, however, the phenomena of laryngeal stenosis more often require surgical intervention (including tracheotomy).
Recurrent respiratory papillomatosis is the most common benign tumor of the larynx in childhood. The first symptom of the disease is usually gradually progressive hoarseness. Later, laryngeal stenosis occurs. Due to the fact that this disease in the initial stages (without endoscopic examination) is often mistaken for laryngitis, the physiotherapeutic treatment given gives impetus to the rapid growth of the tumor. After surgical removal of papillomas, the tumor recurs in the vast majority of cases, which requires repeated surgical interventions. Dysphonia develops both as a result of the growth of papillomas and as a result of repeated operations, often leading to the development of cicatricial stenosis in the vocal folds. To prevent iatrogenic dysphonia in recurrent laryngeal papillomatosis, it is necessary, if possible, to remove papillomas without damaging the surrounding intact tissue; during endoscopic laser surgery, use a micromanipulator, set the lowest parameters for power and exposure of laser radiation. Endolaryngeal phonophoresis with cytostatics (prospidin) is used as anti-relapse therapy for recurrent respiratory papillomatosis; cryosurgery; long-term (for six months or more) systemic interferon therapy (reaferon, viferon) and other treatment methods. For older children with a long (several months) inter-relapse period, phonopedic treatment is indicated to prevent additional social maladjustment.
Acquired scar stenosis of the larynx causes dysphonia when the scar is localized in the vocal folds or when the airway lumen is completely obstructed by scar tissue. Treatment tactics for scar membranes localized in the vocal folds are similar to treatment for congenital commissural synechiae. In other cases, depending on the extent, localization of the scar and the diameter of the remaining lumen of the respiratory tract, various, often multi-stage reconstructive operations are required, followed by voice rehabilitation.
Based on the above-mentioned most common causes of dysphonia in children, we recommend the following tactics for voice rehabilitation in children:
- thorough endoscopic examination under local or, if necessary, general anesthesia;
- treatment of identified concomitant diseases (in particular, neurological disorders, gastroesophageal reflux, etc.);
- children of any age with vocal fold nodules or functional dysphonia are indicated for correction of neurological and/or psychological defects and compliance with the vocal regime; phonopedic treatment (which is advisable to combine with inhalations of alkaline and oil solutions and physiotherapy [ultrasound therapy on the larynx area with vocal fold nodules, diadynamic currents on the larynx area with functional dysphonia, magnesium and bromine electrophoresis on the collar area with mutational dysphonia and concomitant vegetative-vascular dystonia etc.]) can only be used by patients 7-8 years of age and older, which is due to the mental characteristics of preschool children (the necessary conditions for phonopedia are the ability to concentrate, perseverance, the ability to independently consolidate acquired skills, etc.);
- the question of the indications and timing of microsurgical endoscopic intervention in children with vocal fold nodules must be decided individually and it is advisable to delay until puberty due to their possible “self-destruction.” In the meantime, for example, some kind of conservative treatment;
- in children with cysts or polyps of the vocal folds, phonopedic treatment should be preceded by endolaryngeal microsurgical intervention;
- for children suffering from recurrent respiratory papillomatosis, phonopedic treatment is indicated for a long period between relapses;
- in children with cicatricial stenosis of the larynx, surgical treatment should be combined with subsequent phonopedic therapy after restoration of respiratory function
Yu. L. Soldatsky, Doctor of Medical Sciences E. K. Onufrieva MMA named after. I. M. Sechenov, Children's City Clinical Hospital of St. Vladimir, Moscow
When should you call an ambulance?
If your baby has a hoarse voice, you should first determine whether you can cope with the situation on your own or whether you need to call emergency help. You should not take risks and waste time if a hoarse throat is accompanied by the following symptoms:
- The baby developed a barking cough without sputum discharge. A barking cough is paroxysmal in nature, the child cannot “clear his throat” and suffocates during a coughing attack;
- it is difficult for the child to breathe, and a whistle can be heard during inhalation;
- the skin between the ribs noticeably retracts during inhalation;
- the baby has difficulty swallowing;
- hypersalivation is observed, that is, salivation increases;
- The baby's nasolabial triangle turns blue. This symptom indicates that the amount of oxygen in the blood is sharply reduced, and the baby is at risk of hypoxia.
It is important to remember that signs of suffocation in infants should never be ignored, even when the disease occurs without fever.
This is due to the fact that the larynx in newborns is narrow and quickly closes when the surrounding tissues swell, and the brain is extremely sensitive to hypoxia.
Treatment
Treatment of newborn children should be as careful as possible and under the supervision of a doctor (so as not to harm the baby’s health), since most medications are contraindicated at this age.
So, experts recommend limiting yourself to the following drugs:
- Paracetamol (if body temperature is above normal). Approximate dosage: 1/3 tablet, pre-dissolved in warm water (give no more than 2-3 times a day).
- Suprastin for intravenous injection (if the cause of a hoarse voice is an allergic reaction). Daily dose: 5 mg.
- Ambrobene syrup (for severe cough). Give half a measuring cup 2 times a day.
- Anaferon for children (drops for oral administration). The remedy is indicated in cases where there is a viral infection of the upper respiratory tract. Approximate dosage: 10 drops several times a day.
- Inhalipt spray (for sore throat). Spray into the mouth 3-4 times a day.
Important! Self-medication can be dangerous for a child’s health, so before using any drug, it is recommended to consult with your pediatrician.
The specialist will select a safe dosage.
What to do if your child’s voice is hoarse?
What to do if a newborn has a hoarse voice?
The following recommendations should be followed:
- seek medical help. If emergency assistance is not required, you need to call a local pediatrician, who will determine the reasons why the child lost his voice;
- To alleviate the child’s condition, you should humidify the air in the room using a special device. If a humidifier is not available, you can lay wet towels on the central heating radiators. The child should be given warm water to drink (of course, if he is not choking) or warm milk with honey. Water or milk should not be too cold or, on the contrary, too hot: this can lead to even more severe irritation of the larynx. Other drinks - juices, compotes, fruit drinks - are prohibited.
The doctor's recommendations should be followed strictly. Self-medication for a number of diseases that cause hoarseness can be dangerous
First aid
Red dots on the palate of a child, fever, redness of the throat
In addition to calling a doctor, parents should know what to do if their baby becomes hoarse and develops worrying symptoms.
It helps with laryngospasm if the baby breathes moist air. It is recommended to use an industrial humidifier; if you don’t have one, you can take the child to the bathroom, close the door tightly and open the hot water tap. If the baby can drink, it is recommended to give him warm water.
First aid for false croup
Important! It is forbidden to give your baby sweet juices or compotes, as well as chilled or too hot drinks, as this can cause irritation of the larynx.
How to provide emergency assistance if a foreign body gets into the larynx?
It is very important for parents to remember that if a foreign body blocks the baby’s airways, they should act immediately. If threatening symptoms appear, then delay may cost the infant his life. Therefore, you should remember the first aid algorithm when any object gets into the baby’s windpipe:
We recommend reading: How to treat a cough in an infant
- Turn the baby upside down. Hold him by the legs and tap him on the baby's back. It is important to remember that these actions should be performed over a chair or soft sofa. Otherwise, you risk causing additional injury to your baby if you fall;
- Sit down and place the baby with his tummy on your left knee. In this case, the left hand should support the child under the chest and neck. The baby's legs must be tucked under the armpit. Using your palm, apply several sharp, jerky blows to the child’s back between the shoulder blades. In this case, blows should be applied in the direction of the baby's head.
If a foreign object flies out of the child’s throat, but breathing disappears or has not been restored at all, resuscitation should be started. It is important to remember that this is a baby and the lung capacity of an infant is less than that of an adult. Therefore, the volume of one breath into the child’s nose should be equal to the volume of air that an adult “takes” into his mouth, slightly inflating his cheeks. After each inhalation, you need to make five compressions on the chest, pushing the heart area about 2 centimeters. The fact that breathing has been restored is indicated by the presence of a pulse, as well as the restoration of the pink color of the baby’s skin.
How to treat a missing voice
In this situation, much depends on the cause of dysphonia or aphonia. The age of the patient should also be taken into account - treating a hoarse voice in an adult will have to be different than restoring it in a child: treatment methods, doses of drugs, and the drugs themselves are different.
Infectious causes
If it is already known that the cause is a cold, the missing voice should be treated in a comprehensive manner. First of all, you need to create conditions of high humidity - local immune factors are better at killing viruses on the mucous membrane that is moistened from the outside. Due to inflammation at the beginning of the process, it dries out, which is why the voice disappears. The humidity in the apartment is increased with the help of special air humidifiers, although a wet sheet thrown over the heating radiator will do. You can even place a bowl of water in the room. For the same purpose, it is recommended to drink plenty of warm drinks (cold and hot drinks can increase swelling of the mucous membrane of the respiratory tract).
You can also humidify the inhaled air through inhalation. It is ideal to use saline nebulizers for 10-15 minutes. It is also possible to simply inhale the steam of potato broth or soda-salt steam inhalation (you just need to let the water cool a little so that the steam is not hot).
If an adult or child has a hoarse voice, be sure to establish a voice rest regime. A complete refusal to talk (in emergency cases, whispering is allowed) will allow the vocal cords to “rest” and recover faster.
As for medications, you can take any mucus-thinning drugs, starting with regular thermopsis tablets and ending with ambroxol, bromhexine, ACC and the like. In case of a bacterial infection, it is necessary to prescribe antibiotics (a doctor will be able to distinguish bacterial inflammation from viral inflammation; you can make an appointment on our website dobrobut.com).
Non-infectious causes
Treatment is usually carried out on an outpatient basis. Hospitalization is recommended when other signs of illness develop along with a change in voice. Breathing disorders and increased intoxication are alarming symptoms that need to be treated in a hospital setting. In addition, hospitalization is indicated for cancer, myasthenia gravis, chemical and thermal burns of the upper respiratory tract, severe forms of allergies, and laryngeal injuries. In these cases, intensive care, resuscitation measures, and even surgical treatment may be necessary. The following medications can be used in therapy:
- corticosteroids (prednisolone, dexamethasone) to suppress allergies or excessive immune reactions to a foreign agent;
- desensitizing antihistamines (for the same purpose);
- vitamins;
- sedatives.
If signs of suffocation occur simultaneously, the patient can be intubated and connected to an artificial respiration apparatus, while the inhaled air is enriched with oxygen and humidified.
If severe swelling of the larynx develops, a cricoconicotomy or tracheotomy is performed (in other words, the throat is cut and a breathing tube is inserted into it), which will allow the patient to breathe despite the disease blocking the windpipe.
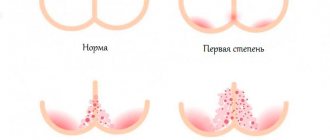
A child has a hoarse voice when crying for a long time
One of the reasons for hoarseness in young children is prolonged screaming. It negatively affects the sensitive tissues of the larynx, as a result of which swelling of the ligamentous apparatus develops, and small bubbles appear in the soft tissues. Parents often believe that there is nothing wrong with this - neither prolonged crying, nor a change in the timbre of the voice. But this is not so - in children at this age, all processes of the nervous system are unstable, and the structures of the larynx are not mature enough and are tender, so a hoarse voice appears for a long time, in addition, nervous disorders often develop in the form of various neuroses.
Persistent hoarseness with frequent crying and/or intense screaming against the background of insufficiently formed vocal cords is associated with the formation of specific protrusions on their surface in the form of small nodules, which prevent them from tightly closing with constant vocal strain.
In the future, this can cause frequent manifestations of colds and viral infections in the form of laryngitis and “false croup,” which is extremely dangerous in children of early and preschool age.
Therefore, parents need to remember that they should not allow their baby to cry and scream for no reason - this may negatively affect his health in the future.